
NEUROMUSCULAR DENTISTRY (originally published in the American Equilibration Society magazine)
Ira L Shapira DDS, DABDSM, DAAPM, FICCMO
These are Video Testimonials of TMJ and Orofacial Pain Patients Treated By Dr Shapira: https://www.youtube.com/channel/UCk9Bfz6pklC7_UluWFHzLrg/videos
Neuromuscular Dentistry remains an enigma to many dentists who do not understand the purposes of the electrodes, the TENS, the computers and more. It has unfairly become a target of poor and misleading definitions by doctors who do not understand its basic principles.
There are several basic premises that underlie Neuromuscular Dentistry. The first premise is that the stomatognathic muscles are the primary determinate of the mandibles position during all jaw functions (when the teeth are not in occlusion) and that rest position is one of the most important positions in dentistry. Rest position is a maxillary to mandibular jaw relation where the teeth are not in occlusion but are prepared to occlude. In Neuromuscular Dentistry Rest is a position of bilaterally equal and low muscle tonicity from which the mandible moves into full occlusion with minimal muscle accommodation. Following closure from rest position the mandible should return to rest with similarly balanced low muscle tonicity. Rest position is determined not only by the mandible’s relation to the cranium but also by the position of the head relative to the body, the suprahyoid and infrahyoid muscles and the position of the hyoid bone. To fully understand the relation of jaw movement to head posture read the Quadrant Theorem of GUZAY (Available from the ADA Library). In essence it shows in engineering terms that after accounting for both rotation and translation of the mandible the actual axis of rotation of the mandible is at the odontoid process of the second vertebrae not at the mandible condylar head.
The second premise is that occlusion is important in neuromuscular dentistry as a resetting mechanism of the trigeminal nervous system’s control of the stomatognathic muscles. Myocentric occlusion is ideally a position in which the muscles move the mandible from a non-torqued rest position into full occlusion with minimal muscle accommodation and no interferences of occlusal contacts until full closure is attained thus eliminating all torque during closure. This means that there are no noxious contacts received by the periodontal ligaments or the muscular proprioceptors that must be avoided by the muscles (accommodation) but rather allow “free” entry into myocentric occlusion. The jaw muscles will return to rest position after closure with the muscles maintaining their healthy low tonicity. Relaxed healthy musculature is the gold standard of neuromuscular dentistry.
Swallowing is a primary activity when the jaw is closed into full occlusion. In order to swallow it is necessary to fixate the mandible and this happens as the teeth occlude. During chewing, speaking and other jaw functions the teeth do not actually occlude in normal function but are separated (during chewing by a bolus of food). Typically swallowing occurs approximately 2000 times a day and is momentary accounting for 6-10 minutes maximum time in occlusion over the course of the day and acts as a neuromuscular reset switch for trigeminally innervated muscles. During a healthy swallow the teeth will move freely without interference into full occlusion with bilateral equal contact and bilateral equal muscle activity and then return to rest position with low muscle tonicity. A deviate swallow as evidenced by scalloping of the tongue is a sign of a possible TMJ disorder and is also 80% predictive of sleep apnea (80% predictive in Dental study- 70% predictive ENT study)
Neuromuscular occlusion (myocentric) occurs when centric occlusion (maximum non-torqued intercuspation of teeth) is coincidental with a balanced muscle closure where the muscles will return to their relaxed state following closure. Myocentric is the ideal position for swallowing.
The dentist utilizing neuromuscular techniques does not determine a specific position of the condyles in the fossa. The position of the disk and condyle are determined primarily by the teeth (bite or orthotic during occlusal correction therapy) in occlusion (myocentric) and the application of muscle activity. Neuromuscular dentistry allows the patients healthy relaxed muscles to determine the joint relations with the teeth serving as a neuromuscular reset switch during closure. Neuromuscular dentistry rejects the notion that manipulation of the patient’s jaw by the intervention of the clinician muscles are more important in determining the relation of the components of the TM Joint than the muscles of the patient. Centric relation is not used as a reference position for mounting casts on an articulator. Centric Relation is considered a border movement of the mandible and as reported in orthopedic literature joints are rarely used in their border positions.
The HIP plane (defined by hamular notches, incisive papilla and the occipital condyles) and/or Campers plane is used to relate the maxilla to an articulator. When cosmetic considerations are involved photos are used to to incorporate this physiologic plane to soft tissues of the face. Ideally the occlusal plane (parallel to the HIP Plane) will bisect the odontoid process of the axis of the atlantoaxial joint the actual center of rotation for the mandible after accounting for translation and rotation according to the quadrant theorem.
This occlusal plane will be at a 90-degree angle to gravitational force when the head is in an upright position. A neuromuscular bite is used to mount the
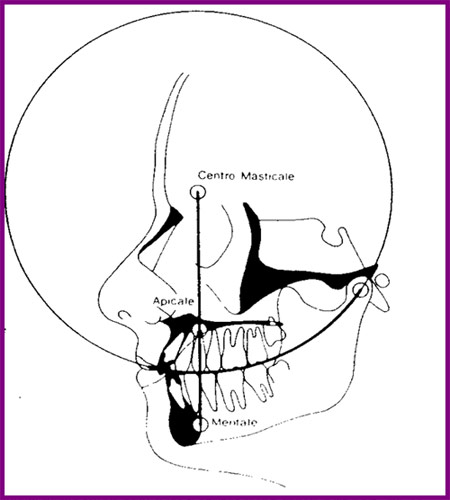
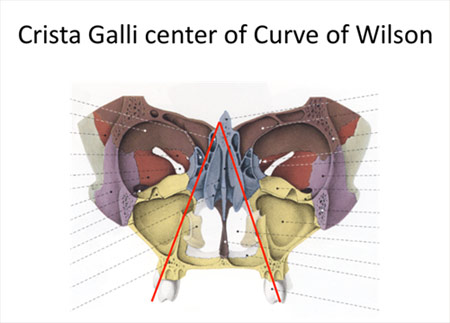
mandibular casts according to data from EMG recordings and jaw tracings with TENS. The incorporation of the Curve of Spee based on Centro Masticale (CM) point which continues thru the mandibular condyle and the Curve of Wilson also based on CM point that is involved is stimulation of the autonomic nervous system via tongue reflexes when the lateral border of the tongue touches the lingual surfaces of the teeth. (Critical Reviews in Oral Biology & Medicine, Vol. 13, No. 5, 409-425 (2002)) This excellent article is available online at http://cro.sagepub.com/cgi/content/full/13/5/409
Neuromuscular dentistry considers many of the problems associated with TMD to be repetitive strain injuries. Movements become harmful when closure requires excessive accommodation and then the system fails at its weakest link. If the weakest link is muscle health we will see formation of tender sore muscles with eventual formation of taut bands and trigger points. If there is muscle overuse from clenching and/or grinding there will be post exercise pain secondary to anaerobic lactic acid build-up. If the weakest point is in the TM Joint then when repetitive strain occurs the muscle accommodation will lead to increased intra-articular pressure. This again will break down the joint at its weakest point. This may occur as a displaced disk or as wear of articular surfaces or many other conditions. It may come at the expense of the bone of the condyle leading to flattening or beaking of the condyle. Clenching and bruxism are two particularly well-known and harmful parafunctional habits that lead to varied repetitive strain injuries. There are many other parafunctions that can lead to problems. Some parafunctions are actually protective muscle accommodation such as the deviated or reversed swallow that protects the TM Joints and masticatory muscles at the expense of altered head, hyoid and spine position and consequent muscle problems.
The second type of problems would be described as I/O or Input/ output errors in computer lingo. The CNS is essentially a biological computer and is affected by input from afferent nerves from the body. Autonomic system function include the fight or flight response with concomitant release of adrenaline that alters the heart rate, blood pressure, muscle tone etc. This system effects the Hypothalamus pituitary complex with feedback to the adrenals and effects on ACTH and cortisol levels. During periods of acute stress these effects have a positive survival value but during chronic stress become a liability to the individual as described by Hans Selye in his book “The Stress of Life” and his discussion of the General Adaptation Syndrome. There are numerous biochemical changes that occur in the brain secondary to aberrant or nociceptive input into the brain these can be affected by correction of the neurological input, by using drugs to change the brain chemistry or a combination of these approaches. Ideally correction of the underlying cause of these biochemical changes is the preferred method of treatment.
The utilization of TENS or transcutaneous neural stimulation over the coronoid notch has been shown by Mitani and Fujii (1974 J. Dent Res.) to block the motor division of the trigeminal nerve and relax the musculature via anti-dromic impulses (hyperpolarisation) to both the alpha and gamma motor neurons without influence from proprioceptive and nocioceptive (tooth contacts) inputs The TENS is then use to create a balanced synchronize pulsing to find the trajectory of closure where a myocentric registration can be obtained. The muscles will return to their relaxed position following closure into myocentric.
The use of Computerized mandibular jaw tracking allows the dentist to measure and record resting jaw position relative to the cranium at a given head position. The location of myocentric occlusion is determined by the dentist with the aid of information from tracings recorded.
Electromyography or EMG is used to record relative values of resting muscle activity of masticatory muscles as well as muscles such as Sternocleidomastoid or Trapezius. While there are no absolute “normal values” of resting muscles the clinician uses his information to compare muscle activity within a given patient. Muscles should be approximately equal activity bilaterally. Thomas 1990 in Frontiers of Oral Physiology vol 7 pp162-170 demonstrated that Spectral analysis of the post TENS EMG may be utilized to evaluate muscle fatigue and differentiate between muscle atrophy or fatigue or relaxed muscle states. This was later confirmed by Frucht, Jonas and Kappert at Frieberg University in 1995 (Fortschr.Kieferorthop vol 56 pp 245-253)
Utilizing the two modalities together allows the clinician to evaluate the rest position of the jaw and simultaneously the health and functional activity of the muscles.
The EMG also allows tests to evaluate the functional capacity of the muscles and again compare the right and left sides for symmetry. The use of functional recordings (during clenching and closure into centric occlusion) allows the clinician to evaluate whether or not muscle function is satisfactory and functional. The use of EMG also allows evaluation and correction of first contact of closure position within microseconds bases on firing order of the masseter and temporalis muscles. The first point of contact on closure is vitally important and equilibration of orthotics and dentition must be finely adjusted until first contact is evenly dispersed on posterior dentition.
Neuromuscular dentistry is very concerned with the effects of mandibular position on the body as a whole and on the effects of the body on jaw and head position. The work of Sherrington and the righting reflex explains how ascending and descending disorders affect a patient. These phenomena have been best explained by Norman Thomas BDS, PhD. I will not attempt to explain this complicated topic in this agenda, which may be found in Anthology of ICCMO vol V pp159-170. It obviously must incorporate the Quadrant Theorem of Casey Guzay, the physiological aspects of the balance organ of the inner ear and the vestibular apparatus located in the brainstem as well as visual feedback. The control of sympathetic and parasympathetic systems by the cerebellum is quite intricate and also affected by head position.
Correction of the chewing cycle is an important part of occlusal finalization. It must be understood that the chewing cycle is different on the each side and that interferences can occur on both the opening and closing strokes of the chewing cycle. Interferences in chewing strokes are easiest to detect by study of the chewing strokes on computerized mandibular scans (MKG). Head position during chewing is not is normally in the upright head position but in the feeding position approximately a 30-degree anterior head flexion. Correction of the chewing cycle is at least as important as correction of right, left and protrusive excursions. Chewing is a healthy function of the craniomandibular apparatus where as excursive movements are actually exercises in parafunctional movements.
There is more commonality to treatment of TMJ disorders by neuromuscular and non-neuromuscular dentists than differences and complications caused by neural intensification in the reticular activating system, emotional aspects and the relation to the limbic system, connections to the sympathetic and parasympathetic nervous systems via the Sphenopalatine Ganglion and sympathetic chain, and chemical changes and cerebroplastic changes that occur during chronic pain leading to hyperalgesia and allodynia all can be discussed in greater detail and explained in relation to neuromuscular dentistry. The basics physiology including effects of Golgi tendon organs and muscle spindles on jaw muscles remain constant and must always be carefully considered during treatment.
Barney Jankelson’s famous quote, “if it is measured it is a fact otherwise it is an opinion “ rings as true today as when he first said it. Neuromuscular dentistry is about making accurate measurements and the use of those measurements to improve the doctor’s ability to make a differential diagnosis and tailor treatment to relieve pain and create stable restorative dentistry with healthy relaxed musculature.
I would like to make a disclaimer that this is my personal definition of Neuromuscular dentistry from 30 years of practice and to thank my mentors Barney Jankelson, Barry Cooper, Dayton Krajiec, Richard Coy, Harold Gelb, Peter Neff, Robert Jankelson and especially Jim Garry who first made me understand the connections between increased upper airway resistance and the common developmental aspects of sleep apnea and craniomandibular disorders. A special thank you for Dr Norman Thomas for his extraordinary help in understanding the complex physiology and anatomy underlying neuromuscular dentistry and in reviewing this paper prior to presentation.
My personal research in the 1980’s as a visiting assistant professor at Rush Medical School examined the jaw relations of patients with obstructive sleep apnea based on neuromuscular evaluations of jaw relations with a Myotronic’s kinesiograph and a myomonitor to find neuromuscular rest position. These studies showed jaw relations in the male apnea patients that were strikingly similar to those found in female TMD patients. The National Heart Lung and Blood Institute considers sleep apnea to be a TMJ disorder. The NHLBI published a report, “Cardiovascular and Sleep Related Consequences of TMJ Disorders” in 2001 that can be found at https://tmj.org/wp-content/uploads/2021/06/NHLBI-sleep-study.pdf
Dr Shapira returned to Rush as an assistant professor at the sleep center in the 1990’s where he treated a wide variety of obstructive apnea patients with commercial and customized intraoral sleep appliances. He was a founding and credentialed member of the Sleep Disorder Dental Society that has become the American Academy of Dental Sleep Medicine, He is a Diplomate of the American Board of Dental Sleep Medicine, on the board of the Illinois Sleep Society, a Diplomat of the American Academy of Pain Management, a Regent Fellow of the International College of Cranio-Manibular Orthopedics and a representative of that group to the TMD Alliance. He is a long time member of AES, AACFP, Academy of Sleep Medicine and the Chicago Dental Society. Dr Shapira teaches hands-on in-depth Dental Sleep Medicine courses to small groups at his Gurnee office. A family history of genetic cancer led Dr Shapira into research on stem cells an he also holds several patents (method and device) on the collection of stem cells during early minimally invasive removal of the uncalcified tooth bud of developing third molars. This procedure can be complete in minutes with greatly reduced morbidity compared to current surgical techniques used for removal of developed third molars. He hopes in the future that patients will routinely remove the tooth buds and collect and save the stem cells for anti-aging and regenerative medical uses.
For more information on headache diagnosis and treatment as related to neuromuscular dentistry, please visit our, I Hate Headaches Website or my Think Better Life website.
![]()